
Introduction:
By July 23rd, 2020 there were 15,117,078 SARS-CoV-2 infections, resulting in 620,033 deaths.
Prompted by the unrelenting progress of the pandemic, and based upon new research from Beigel et al., the Therapeutic Goods Administration (TGA) announced that remdesivir (“Veklury”, Gilead Sciences Pty Ltd) had received provisional approval as the first treatment option for COVID-19, caused by SARS-CoV-19 (severe acute respiratory syndrome coronavirus). Approval for use is currently restricted to adults and adolescent patients with severe COVID-19 symptoms who have been hospitalised.
Remdesivir (GS-5734), is a nucleoside analogue pro-drug. A nucleoside is comprised of a nitrogen base plus the sugar, ribose, but without the phosphate group (discussed below).
Remdesivir antiviral activity:
SARS-CoV-19 is a member of the coronavirus family. It is an enveloped virus with a positive-sense, single-stranded RNA genome that infects animal species and humans. Other members of this viral family are those responsible for the common cold, severe acute respiratory syndrome coronavirus (SARS) and Middle East respiratory syndrome-related coronavirus (MERS).
In vitro, remdesivir inhibits all human and animal coronaviruses thus far tested, including SARS-CoV-2. It has also shown to have antiviral properties and clinical benefits in animal models of SARS-CoV-1 and MERS infections.
Mechanisms of action of remdesivir:
To understand the mechanism of action of remdesivir, a review of the structural architecture of RNA is warranted.
Briefly, all RNA viruses use RNA-dependent RNA polymerase (RdRP) to carry out the biosynthesis of a new RNA strand from an RNA template.
Like all RNA viruses, SARS CoV-2 RNA is comprised of four nitrogen-containing bases – uracil (U), cytosine (C), adenine (A) and guanine (A). These bases are joined to ribose, a sugar molecule, and a phosphate group, to form what is known as a nucleotide. (Figure 1)
A nucleotide is the foundational building block of nucleic acids. If the phosphate group is absent, the structure is called a nucleoside.
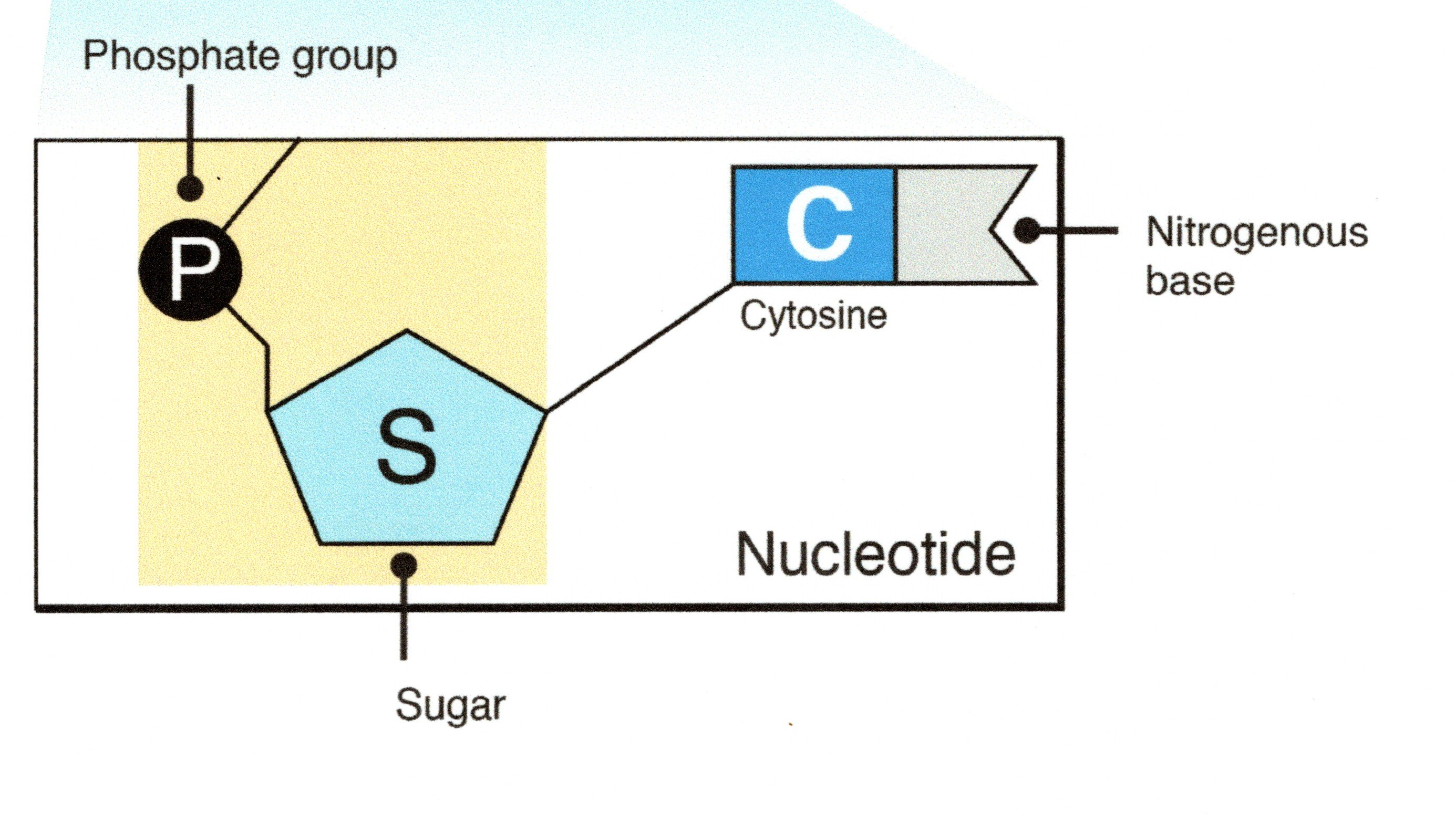
Figure 1. (Courtesy: National Human Genome Research Institute)
During normal viral reproduction, adenine pairs with uracil and cytosine pairs with guanine. This replication is performed by RNA-dependent RNA polymerase (RdRp). As noted earlier, it is the role of RdRp to match the correct corresponding base, to form the correct base pair. (Figure 2)
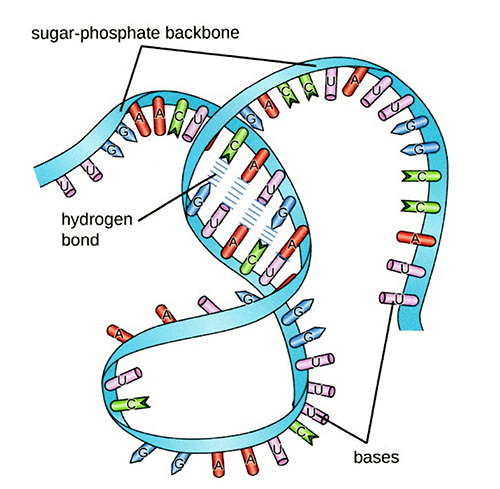
Figure 2. (Courtesy: OpenStax)
There are three methods by which remdesivir blocks RNA viral replication.
The primary mechanism of action of remdesivir (RDV), given as the pro-drug RDV triphosphate (RDV-TP), is to substitute itself for the adenine nucleotide known as adenosine triphosphate (ATP), to which it is structurally similar. (see figure 3).
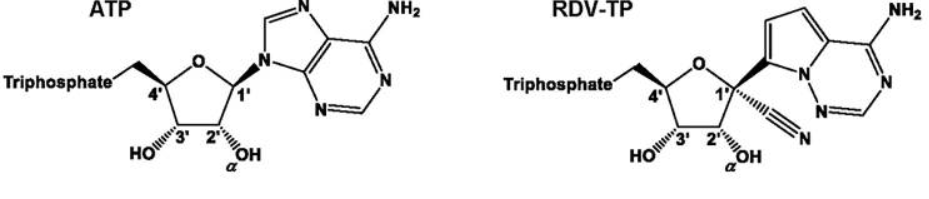
Figure 3 (Courtesy: Gordon et al., J Biol Chem)
RDV then binds to uracil, which results in termination of viral replication due to the false base in the replication chain.
The second important mechanism for RDV is a variation to the carbon-nitrogen (CN) group attached to ribose, the RNA relevant sugar.
This variation means that as RDV is included into the replicating RNA chain, the presence of the CN group causes the chain to become misshaped. This distortion means that only three more nucleotides can be added before viral RNA synthesis is terminated at position i+3, where i is the insertion point of remdesivir in the new RNA chain.
The third important mechanism of action flows from the second. Because three extra nucleotides have been inserted by RdRp into the new RNA strand after the insertion of the RDV “look-alike” base, the presence of RDV may now be protected from removal by the coronavirus’s exonuclease enzyme.
Exonuclease is a feature of coronaviruses which act to recognise and remove (clip out) artificial nucleotides. It is the virus’ proof-reading mechanism. The chemical bond changes mean that remdesivir cannot be excised, resulting in chain propagation with delayed but eventual termination of RNA synthesis. Because RDV has been added into the RNA chain replication, it has stealthily avoided “the proofreading subunit required to safeguard coronavirus replication fidelity.”
Early study “failure” with remdesivir used in treating Ebola.
In trials against Ebola virus in the Democratic Republic of the Congo in 2018, remdesivir was found to be inferior to other comparators in terms of patient mortality and was withdrawn from the study. It was concluded that it was a failure, due to a higher mortality rate from Ebola in recipients when compared to than other trial drugs.
However, the conclusion that it is an ineffective antiviral drug is erroneous. The explanation for RDVs poor performance against Ebola virus but success against SAR-CoV-2 is due to the variation in binding strengths of RDV and adenosine in the two viruses. RDV binds four times less strongly to the Ebola polymerase – the enzyme that makes RNA copies – than does the adenine containing nucleotide, adenosine triphosphate (ATP).
Thus, in the Ebola virus, due to a higher binding efficacy to Ebola polymerase, adenosine takes its correct position and binds to uracil. Consequently, viral replication is not significantly impeded.
However, in COVID-19 patients, RDV binds four times more strongly to SARS-COV-19 polymerase, resulting in the exclusion of the adenosine triphosphate, the inclusion of RDV in its place, and the base pairing of remdesivir – not adenine – to uracil. Consequently, SARS-COV-19 replication is terminated.
Remdesivir study in Hubei.
Patients in this study, conducted from Feb 6, 2020, and March 12, 2020 were randomly assigned in a 2:1 ratio to remdesivir IV (200 mg on day 1, then 100 mg on days 2–10 as a single daily infusion) or a placebo of the same volume (n=237). Both RDV and placebo were given for ten days.
Remdesivir use was not associated with a difference in time to clinical improvement (hazard ratio 1·23 [95% CI 0·87–1·75]), and there was no significant difference in time to clinical improvement between RDV or placebo patients. RDV use was terminated early because of adverse events.
A therapy confounder in this study was that patients were permitted concomitant use of lopinavir–ritonavir, interferons, and corticosteroids.
Clinical support for remdesivir use.
On May 22, 2020, Beigel and co-workers published the results of a double-blind, randomised, placebo-controlled trial of remdesivir (IV) in adults hospitalised with Covid-19 with evidence of lower respiratory tract involvement.
Patients received either remdesivir (200 mg loading dose on day 1, followed by 100 mg daily for up to 9 additional days) or placebo for up to 10 days. The primary outcome was the time to recovery, defined by either discharge from the hospital or hospitalisation for infection-control purposes only.
Preliminary results from the 1059 patients (538 assigned to remdesivir and 521 to placebo) with data available after randomisation indicated that those who received remdesivir had a median recovery time of 11 days (95% CI, 9 -12), as compared with 15 days (95% CI, 13 to 19) in those who received placebo (rate ratio for recovery, 1.32; 95% CI, 1.12 to 1.55; P<0.001).
At 14 days, the Kaplan-Meier estimates of mortality were 7.1% with remdesivir and 11.9% for placebo (hazard ratio for death, 0.70; 95% CI, 0.47 to 1.04).
This reduction in mortality was not clinically significant.
Serious adverse drug events were reported in 114 of 541 patients in the RDV group (21.1%) and 141 of 522 patients in the placebo group (27.0%).
The authors concluded that RDV was superior to placebo in shortening hospitalised COVID-19 adults recovery time who had evidence of lower respiratory tract infection.
Criticisms of the trial:
Correspondents to the New England Journal of Medicine have raised several concerns with the study.
- Samantha Gillenwater, M.D. noted that patients with Covid-19–related respiratory disease, the median time to randomisation was nine days, at which stage the illness was advanced. A more instructive result may have been obtained if RDV had been commenced earlier.
- James H. McMahon, Ph.D considered that RDV may have been given too late to many patients, since the median time to onset of acute respiratory distress syndrome (ARDS) is 8.0 days.
- Julián Olalla, M.D., Ph.D. asked what other medications (hydroxychloroquine, lopinavir–ritonavir, azithromycin, or tocilizumab) were allowed if the local protocols permitted their use.
In reply, Dr Beigel noted that the report was interim data and that further data analysis will address these and other issues raised by colleagues.
Conclusion:
In mid-May 2020 it was estimated that a vaccine would not be out of phase 3 trials until mid-2021. Thus, early use of hydroxychloroquine with zinc and azithromycin, remdesivir or tocilizumab appeared to be the best clinical measures available. However, in late July 2020, at least four research centres reported promising results, with a vaccine now possible in mid-2021. These vaccine candidates include:
- The University of Queensland protein spike clamp,
- Novavax and its trial vaccine, designed to trigger an immune response by imitating the SARS-CoV-2 spike protein,
- The University of Oxford trial vaccine named ChAdOx1 nCoV-19 which was tested in a joint phase 1 and 2 trial of 1,077 people aged 18-55, and
- Moderna have developed an mRNA vaccine which encodes the SARS-CoV-2 spike (S) glycoprotein. The S glycoprotein facilitates host cell attachment and is essential to viral entry into the host cell. Volunteers produced both antibodies against SARS-CoV-2, and immune T cells to the virus. Phase 3 trials begin in the northern summer of 2020.
References:
- Agostini ML, Andres EL, Sims AC, Graham RL, Sheahan TP, Lu X, et al. Coronavirus susceptibility to the antiviral remdesivir (GS-5734) is mediated by the viral polymerase and the proofreading exoribonuclease. mBio. 2018; 9(2): e00221-18.
- Baltaci S. Successful treatment strategy of turkey against Covid-19 outbreak. Brussels: European Commission; 2020.
- Beigel JH, Tomashek KM, Dodd LE, Mehta AK, Zingman BS, Kalil AC, et al. Remdesivir for the treatment of Covid-19 — preliminary report. N Engl J Med. 2020: DOI: 10.1056/NEJMoa2007764.
- Bloom J. Remdesivir should inhibit coronavirus despite failing against Ebola. American Council on Science and Health; 2020.
- Brody L. Nucleotide. Bethesda: National Human Genome Research Institute.
- Carlucci P, Ahuja T, Petrilli CM, Rajagopalan H, Jones S, Rahimian J. Hydroxychloroquine and azithromycin plus zinc vs hydroxychloroquine and azithromycin alone: outcomes in hospitalized COVID-19 patients. medRxiv [Internet]. 2020: 2020.05.02.20080036.
- Department of Health. Australia’s first COVID treatment approved. Woden: Therapeutic Goods Administration; 2020.
- Eastman RT, Roth JS, Brimacombe KR, Simeonov A, Shen M, Patnaik S, et al. Remdesivir: a review of its discovery and development leading to emergency use authorization for treatment of COVID-19. ACS Cent Sci. 2020; 6(5): 672-83.
- Folegatti PM, Ewer KJ, Aley PK, Angus B, Becker S, Belij-Rammerstorfer S, et al. Safety and immunogenicity of the ChAdOx1 nCoV-19 vaccine against SARS-CoV-2: a preliminary report of a phase 1/2, single-blind, randomised controlled trial. Lancet. 2020; S0140-6736(20)31604-4. doi: 10.1016/S0140-6736(20)31604-4
- Gordon CJ, Tchesnokov EP, Feng JY, Porter DP, Götte M. The antiviral compound remdesivir potently inhibits RNA-dependent RNA polymerase from Middle East respiratory syndrome coronavirus. 2020. 295(15): 4773-9.
- Gordon CT, Tchesnokov EP, Woolner E, Perry JK, Fengy JY, Porter DP, et al . Remdesivir is a direct-acting antiviral that inhibits RNA-dependent RNA polymerase from severe acute respiratory syndrome coronavirus 2 with high potency. J Biol Chem. 2020; 295(20): 6785-97.
- Green A. Dosing begins in first human trial of UQ COVID-19 vaccine2020. Canberra: CSIRO; 2020.
- Guo C, Li B, Ma H, Wang X, Cai P, Yu Q, et al. Tocilizumab treatment in severe COVID-19 patients attenuates the inflammatory storm incited by monocyte centric immune interactions revealed by single-cell analysis. bioRxiv [Internet]. 2020: 2020.04.08.029769.
- Jackson LA, Anderson EJ, Rouphael NG, Roberts PC, Makhene M, Coler RN, et al. An mRNA Vaccine against SARS-CoV-2 — peliminary report. New Engl J Med. 2020. DOI: 10.1056/NEJMoa2022483.
- Lewin E. ‘It’s just a race against time’: Developing a COVID-19 vaccine. NewsGP [Internet]. 2020.
- Mackenzie R. DNA vs. RNA – 5 key differences and comparison. Sudbury: Technology Networks; 2018.
- Mulangu S, Dodd LE, Davey RT, Tshiani Mbaya O, Proschan M, Mukadi D, et al. A randomized, controlled trial of Ebola virus disease therapeutics. New Engl J Med. 2019; 381(24): 2293-303.
- Oldach L. Slipping past the proofreader. Rockville: ASBMBToday; 2020.
- Parker N, Schneegurt M, Tu AH, Forster BM, Lister P. Structure and Function of RNA. In: Microbiology. Houston: Lumen Learning.
- Quinn K. Coronavirus vaccine progress report: the projects bidding to win the race for a COVID-19 vaccine 2020. ABC News; 2020.
- Remdesivir for the treatment of Covid-19 — preliminary report. Letters to the Editor. N Engl J Med. 2020.
- Saha A, Sharma AR, Bhattacharya M, Sharma G, Lee S-S, Chakraborty C. Probable molecular mechanism of remdesivir for the treatment of COVID-19: need to know more. Arch Med Res. 2020; 10.1021/acscentsci.0c00489.
- Seley-Radtke K. Remdesivir explained – what makes this drug work against viruses? Parkville: The Conversation: 2020.
- Shu B, Gong P. Structural basis of viral RNA-dependent RNA polymerase catalysis and translocation. Proc Natl Acad Sci USA. 2016; 113(28): E4005-E14.
- Number of coronavirus (COVID-19) cases, recoveries, and deaths among the most impacted countries worldwide as of July 23, 2020 2020.
- Subissi L, Posthuma CC, Collet A, Zevenhoven-Dobbe JC, Gorbalenya AE, Decroly E, et al. One severe acute respiratory syndrome coronavirus protein complex integrates processive RNA polymerase and exonuclease activities. Proc Natl Acad Sci USA. 2014; 111(37): E3900-E9.
- Wang D, Hu B, Hu C, Zhu F, Liu X, Zhang J, et al. Clinical characteristics of 138 hospitalized patients with 2019 novel coronavirus-infected pneumonia in Wuhan, China. JAMA. 2020; 323(11): 1061-9.
- Wang Y, Zhang D, Du G, Du R, Zhao J, Jin Y, et al. Remdesivir in adults with severe COVID-19: a randomised, double-blind, placebo-controlled, multicentre trial. Lancet. 2020; 395(10236): 1569-78.
- Ye W, Yao M, Dong Y, Ye C, Wang D, Liu H, et al. Remdesivir (GS-5734) impedes enterovirus replication through viral RNA synthesis inhibition. Front Microbiol. 2020; 11: 1105.
Subscribe Knowledge Centre Updates
Enter your details to receive Knowledge Centre updates