
Diabetes mellitus is a chronic condition in which the body loses its ability to produce insulin, or begins to produce insulin less efficiently, resulting in blood glucose levels that are too high.
Insulin is a hormone produced by beta cells in the pancreas. It facilitates the uptake of glucose from the bloodstream into the cells. Insulin is essential to prevent the accumulation of glucose in the circulation, which can cause complications such as peripheral neuropathy (nerve damage) and diabetic nephropathy (kidney impairment).
Type 1 diabetes mellitus (T1DM) develops when the pancreas stops producing insulin due to damaged or destroyed beta cells. Without insulin, glucose cannot move from the bloodstream into the cells. People with T1DM are reliant on insulin injections.
Type 2 diabetes mellitus (T2DM) develops when the pancreas cannot make sufficient insulin and/or the body doesn’t respond adequately to the insulin that is produced (insulin resistance). People with T2DM may require insulin injections as the disease progresses.
Types of Insulin
There are five types of insulin available in Australia, categorised based on their onset and duration of action.
Rapid-acting insulin
Rapid-acting insulin starts working between 2.5 – 20 minutes after injection. Its action peaks between one and three hours post-injection and can last up to five hours. This type of insulin is used to facilitate the uptake of glucose after eating as this mimics the body’s natural insulin response. It is injected immediately before meals.
The three rapid-acting insulins available in Australia are:
- NovoRapid® and Fiasp® (insulin aspart)
- Humalog® (insulin lispro)
- Apidra® (insulin glulisine)
Short-acting Insulin
Short and rapid-acting insulins are often referred to as ‘bolus’ insulins due to their shorter duration of action compared to intermediate and long-acting insulins.
Short-acting insulins begin to work within 30 minutes of injection, so need to be administered approximately 30 minutes prior to meals. They reach their maximum effect 2-5 hours later and last for 6-8 hours.
Short-acting insulins available in Australia include:
- Actrapid® (insulin neutral)
- Humulin® R (insulin neutral)
Intermediate-acting Insulin
Intermediate and long-acting insulins are often referred to as ‘basal’ insulins due to their sustained release and longer duration of action.
Intermediate-acting insulins have a cloudy appearance and need to be mixed well prior to administration (normally rolled in the hand).
These insulins begin to work around 60-90 minutes after injection, peak between 4 to 12 hours later and last for between 16 and 24 hours.
Intermediate-acting insulins available in Australia include:
- Humulin NPH® (a human isophane insulin)
- Protaphane® (a human isophane insulin)
Long-acting insulin
Long-acting insulins produce a slow, steady release with no apparent peak in action. They last between 18 and 24 hours and can be administered once or twice daily.
Long-acting insulins available in Australia include:
- Levemir® (insulin detemir)
- Tresiba® (insulin degludec)
- Optisulin® (insulin glargine 100iu/mL) *As of July 2020 Lantus® was discontinued and replaced with Optisulin® (insulin glargine 100iu/mL)
- Toujeo® (insulin glargine 300iu/mL)
It is very important to note the difference in concentration between Optisulin® and Toujeo®, as they are both insulin glargine. They are not interchangeable.
Due to the high risk of error associated with the prescribing and administering of insulin, it is required that insulins are prescribed using their brand names; this reduces the risk of accidentally administering a three times stronger insulin glargine than was intended.
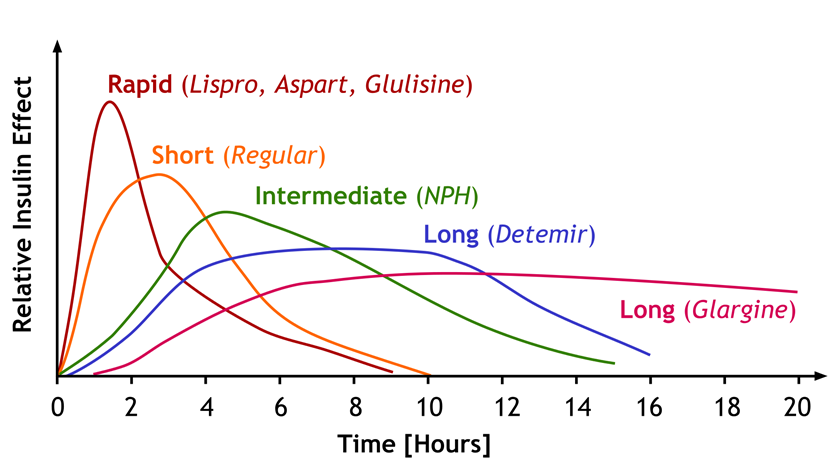
Figure 1: Duration of action of different insulin classes (Image by Peters, licensed under CC BY 3.0)
Mixed Insulin
Mixed insulins contain a pre-mixed combination of either very rapid-acting or short-acting insulin, together with intermediate-acting insulin.
The mixed insulins currently available in Australia include:
- Rapid-acting with intermediate-acting insulin:
- NovoMix® 30 (30% rapid, 70% intermediate protaphane)
- Humalog® Mix 25 (25% rapid, 75% intermediate Humulin® NPH)
- Humalog® Mix 50 (50% rapid, 50% intermediate Humulin® NPH)
- Short-acting and intermediate-acting insulin:
- Mixtard® 30/70 (30% short, 70% intermediate protaphane)
- Mixtard® 50/50 (50% short, 50% intermediate protaphane)
- Humulin® 30/70 (30% short, 70% intermediate Humulin® NPH)
- Rapid-acting and long-acting insulin:
- Ryzodeg® 30/70 (30% rapid, 70% long-acting degludec)
Basal Bolus Insulin Dosing
Basal bolus insulin dosing is designed to reflect the activity of endogenous insulin i.e. the availability of small amounts of insulin throughout the day, with peaks released in response to meals.
Sliding Scale Insulin Dosing
Sliding scale insulin dosing is often used in the hospital setting. It involves variable bolus doses of rapid-acting insulin based on pre-meal blood glucose levels. Basal insulin doses remain unchanged.
Sliding scale insulin regimens are not common outside of the acute setting, however some people do use them to enable tight control of blood glucose levels.
High Risk
Insulin is considered a high-risk medication due to its ability to cause severe complications if administered incorrectly (intravenous or intramuscular instead of subcutaneously) or in the incorrect dose (mL instead of units) or at the wrong time. Such complications include hypoglycaemia (which can lead to loss of consciousness and death), hyperglycaemia, and diabetic ketoacidosis.
References:
- Australian Commission on Safety and Quality in Healthcare. High risk medicines resources. Sydney: ACSQHC; 2019.
- Better Health Channel. Diabetes and Insulin. Melbourne: State Government of Victoria; 2019.
- Rossi S (editor). Insulins. In: Australian Medicines Handbook. Adelaide: AMH; 2020.
Subscribe Knowledge Centre Updates
Enter your details to receive Knowledge Centre updates